 RSS Feed
RSS Feed

















 November 8th, 2021
November 8th, 2021  Awake Goy
Awake Goy By The Exposé on
The purpose of government Covid-19 statistics is no longer to inform the public with scientific truth, in order to help them formulate a valid medical decision on the risks and benefits of Covid-19 Vaccines.
It is to influence the public with misleading or false or politically biased or medically biased information and to suppress any information which does not suit their political agenda in order to effectively make that choice for them.
By a concerned reader
On November 2nd, the Daily Mail published an article revealing that…
1. UK statistics watchdog scolds PHE’s replacement body for publishing ‘misleading’ figures which anti-vaxxers have seized as proof that Covid jabs don’t work
2. Over the past few weeks, the agency’s data shows infection rates are higher in fully-vaccinated adults compared to the unjabbed.
3. Anti-vaxx commentators and campaigners have seized the data as proof that Covid vaccines don’t work.
The UK’s Statistics Watchdog is The Office of Statistics Regulation (TOSR for short). Yes Offstats has told the UKHSA that their Stats are off. And now they are nicely back on message.
TOSR director general Ed Humpherson wrote to the UKHSA’s boss Dr Jenny Harries on November1 thanking her for the changes she had made and is quoted in the Daily Mail as saying
‘It remains the case that the surveillance report includes rates per 100,000 which can be used to argue that vaccines are not effective,’
‘I know that this is not the intention of the surveillance report, but the potential for misuse remains.
There is the tacit admission by the Government that the purpose of their stats is not to enable the public to decide for themselves whether the vaccines are effective or not. No their stats should not even be able to support an argument that the vaccines are ineffective. Indeed any such construction of UKHSA statistics would be a misuse of government data according to the Director General.
This is his candid admission that the use of all UKHSA data is exclusively to prove the vaccines are effective, and any government statistics agency which departs from that line shall be re-adjusted by TOSR. He is defining the UKHSA as a pro vaccine propaganda outfit, whose mandate is only to supply information for one side of the debate. No person in the UK can be expected to make an informed choice of whether to take Pfizer’s experimental gene therapy when it is presented to them by the government as an unquestionably effective Covid vaccination.
https://www.dailymail.co.uk/health/article-10155799/Stats-watchdog-scolds-PHE-replacement-data-misuse-supports-anti-vaxxers.html‘
The writer therefore calls on Ed Humpherson, to –
1. Withdraw his instruction to the UKHSA to only present data that supports vaccination and to suppress data that has the capability of being used to support vaccine refusal. Because the law requires that the public are given the opportunity to give an informed consent for all medical interventions.
2. To publish forthwith under a Freedom of Information Request, Any and All instructions to other government agencies to the same purpose, namely of influencing the public with one sided propaganda, rather than informing it in a balanced manner with both sides of the argument.
3. To publicly withdraw all such instructions and start presenting the truth to the British people and trust them to make the best decision for themselves, their families and their children.
Here is the latest UKHSA data from their Vaccine Surveillance Report for Week44.
Cases reported by specimen date between week 40 & 43 2021 – https://assets.publishing.service.gov.uk/government/uploads/system/uploads/attachment_data/file/1031157/Vaccine-surveillance-report-week-44.pdf
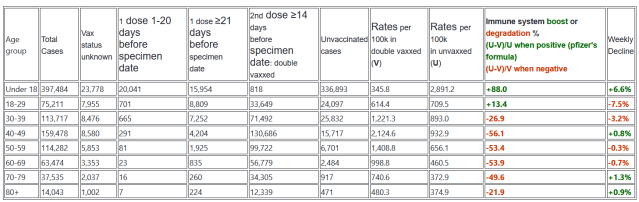
Here is how it fits into the previous 8 weeks of data.
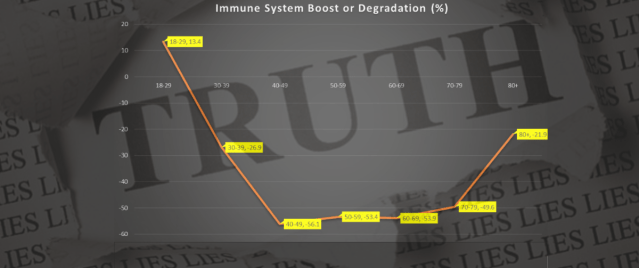
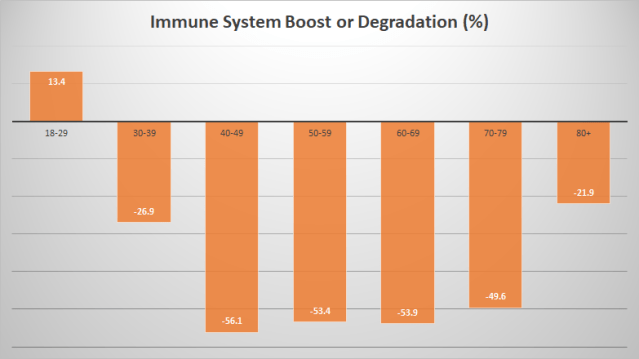
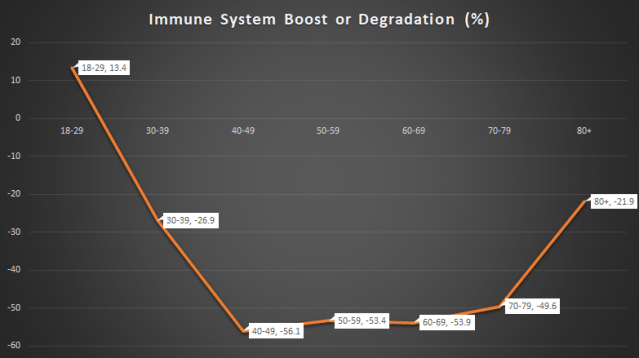
The table below shows the weekly decline in doubly vaccinated immune system performance compared to unvaxxed people. Vaccine efficacy is measured using Pfizer’s vaccine effectiveness formula…
(Unvaxxed case rate – Vaxxed case rate)/the Larger of Unvaxxed or Vaxxed case rate – We are using the normalised absolute ratio of vaxxed to unvaxxed case numbers to determine vaccine efficiency just as Pfizer itself does.



And now, as if by magic, the consistent pattern of the 7 weeks from week35 – week41, has miraculously slowed down and stopped altogether. Well Hallelujah – we are delivered from vaccine induced AIDS coincident with a scolding by the government of its statistics agency.
The writer is not buying this miracle cure and is still projecting the same result that the unmassaged data from Weeks35-41 predict, namely…
The 8 UK PHE Vaccine Surveillance Report figures on Covid cases from Week35-42 showed that doubly vaccinated 40-79 year olds had lost lost 50% of their immune system capability by October 24 and are consistently losing a further 4-5% every week (between 3.7% and 7.9%). Not withstanding what we understand to be the corrupted figures for Week43, we continue to project that 30-49 year olds will have zero Covid/viral defence at best, or a form of vaccine mediated AIDS at worst, by the first week in January and all doubly vaccinated people over 30 will have completely lost that part of their immune system which deals with Covid in the next 17 weeks.
Meanwhile in other news, which you will not be hearing about from any UK government agency regulated by TOSR, Swedish Researchers have discovered one mechanism through which the Vaccines degrade the immune system.
SARS–CoV–2 Spike Impairs DNA Damage Repair and Inhibits V(D)J Recombination In Vitro – https://www.mdpi.com/1999-4915/13/10/2056/htm
by Hui Jiang and Ya-Fang Mei
Department of Molecular Biosciences, The Wenner–Gren Institute, Stockholm University, SE-10691 Stockholm, Sweden and Department of Clinical Microbiology, Virology, Umeå University, SE-90185 Umeå, Sweden
Abstract
Severe acute respiratory syndrome coronavirus 2 (SARS–CoV–2) has led to the coronavirus disease 2019 (COVID–19) pandemic, severely affecting public health and the global economy. Adaptive immunity plays a crucial role in fighting against SARS–CoV–2 infection and directly influences the clinical outcomes of patients. Clinical studies have indicated that patients with severe COVID–19 exhibit delayed and weak adaptive immune responses; however, the mechanism by which SARS–CoV–2 impedes adaptive immunity remains unclear. Here, by using an in vitro cell line, we report that the SARS–CoV–2 spike protein significantly inhibits DNA damage repair, which is required for effective V(D)J recombination in adaptive immunity. Mechanistically, we found that the spike protein localizes in the nucleus and inhibits DNA damage repair by impeding key DNA repair protein BRCA1 and 53BP1 recruitment to the damage site. Our findings reveal a potential molecular mechanism by which the spike protein might impede adaptive immunity and underscore the potential side effects of full-length spike-based vaccines.
The significance of this study is not merely that mRNA vaccines prevent your DNA from repairing itself which will cause immunological disorders, cancer and premature ageing. The problem is that the mRNA is going into your cell nuclei. That is straight up gene therapy – not vaccination. mRNA should go directly to the protein assembly plants in your cells called ribosomes, which it should instruct to manufacture the protein spikes. It should not be going anywhere near the cell nucleus. Entering the cell nucleus means it is performing or effectively performing reverse transcription and making itself a part of or an addition to your genetic code.
Basic Immunology
Vaccines work by simulating a viral attack and provoking the immune system into responding as if you have had the virus. They are supposed to train the immune system to the point where you develop natural immunity to the virus. So the argument that vaccine immunity is better than natural immunity could never have been true because vaccine immunity is an inferior form of natural immunity resulting from the body’s immune response to a vaccine generated simulation rather than to a real world infection. The vaccines program your cells to produce the 1273 Amino Acid S1 Spike Protein, which for the sake of completeness is presented below, with 60 amino acids per line..
1 ) MFVFLVLLPLVSSQCVNLTTRTQLPPAYTNSFTRGVYYPDKVFRSSVLHSTQDLFLPFFS
2) NVTWFHAIHVSGTNGTKRFDNPVLPFNDGVYFASTEKSNIIRGWIFGTTLDSKTQSLLIV
3) NNATNVVIKVCEFQFCNDPFLGVYYHKNNKSWMESEFRVYSSANNCTFEYVSQPFLMDLE
4) GKQGNFKNLREFVFKNIDGYFKIYSKHTPINLVRDLPQGFSALEPLVDLPIGINITRFQT
5) LLALHRSYLTPGDSSSGWTAGAAAYYVGYLQPRTFLLKYNENGTITDAVDCALDPLSETK
6) CTLKSFTVEKGIYQTSNFRVQPTESIVRFPNITNLCPFGEVFNATRFASVYAWNRKRISN
7) CVADYSVLYNSASFSTFKCYGVSPTKLNDLCFTNVYADSFVIRGDEVRQIAPGQTGKIAD
8) YNYKLPDDFTGCVIAWNSNNLDSKVGGNYNYLYRLFRKSNLKPFERDISTEIYQAGSTPC
9) NGVEGFNCYFPLQSYGFQPTNGVGYQPYRVVVLSFELLHAPATVCGPKKSTNLVKNKCVN
10) FNFNGLTGTGVLTESNKKFLPFQQFGRDIADTTDAVRDPQTLEILDITPCSFGGVSVITP
11) GTNTSNQVAVLYQDVNCTEVPVAIHADQLTPTWRVYSTGSNVFQTRAGCLIGAEHVNNSY
12) ECDIPIGAGICASYQTQTNSPRRARSVASQSIIAYTMSLGAENSVAYSNNSIAIPTNFTI
13) SVTTEILPVSMTKTSVDCTMYICGDSTECSNLLLQYGSFCTQLNRALTGIAVEQDKNTQE
14) VFAQVKQIYKTPPIKDFGGFNFSQILPDPSKPSKRSFIEDLLFNKVTLADAGFIKQYGDC
15) LGDIAARDLICAQKFNGLTVLPPLLTDEMIAQYTSALLAGTITSGWTFGAGAALQIPFAM
16) QMAYRFNGIGVTQNVLYENQKLIANQFNSAIGKIQDSLSSTASALGKLQDVVNQNAQALN
17) TLVKQLSSNFGAISSVLNDILSRLDKVEAEVQIDRLITGRLQSLQTYVTQQLIRAAEIRA
18) SANLAATKMSECVLGQSKRVDFCGKGYHLMSFPQSAPHGVVFLHVTYVPAQEKNFTTAPA
19) ICHDGKAHFPREGVFVSNGTHWFVTQRNFYEPQIITTDNTFVSGNCDVVIGIVNNTVYDP
20) LQPELDSFKEELDKYFKNHTSPDVDLGDISGINASVVNIQKEIDRLNEVAKNLNESLIDL
21) QELGKYEQYIKWPWYIWLGFIAGLIAIVMVTIMLCCMTSCCSCLKGCCSCGSCCKFDEDD
22) SEPVLKGVKLHYT
Here is the Amino Acid Look up table…

Whereas the SARS-CoV-2 isolated from Ethiopian patients had: genome sizes were 29,860, 29,856, and 29,871 – https://www.ncbi.nlm.nih.gov/pmc/articles/PMC8459669/
There are 3 nucleotides (genome RNA bases) per Amino Acid. So Covid-19 has around 9953 Amino Acids in total. The virus is therefore around 8x larger than its spike protein. Vaccine immunity results from antibodies to the spike protein. Natural immunity results from antibodies to the entire virus. The immune system chops up virus proteins into small sections and produces a different antibody for each section. So natural immunity will produce 8x as many antibody types as virus immunity. This is one reason why it is so much better. In one analysis that compared more than 32,000 people, they found that the risk of developing symptomatic COVID-19 was 27 times higher among the vaccinated, and the risk of hospitalisation 8 times higher – https://thepulse.one/2021/08/29/covid-infection-provides-greater-protection-than-being-fully-vaccinated-new-study/ and https://www.medrxiv.org/content/10.1101/2021.08.24.21262415v1.
Simply put natural immunity is 8x as broad based as vaccine immunity for Covid19 spike protein vaccines.
Vaccines do two things for the immune system. They show it the enemy and they agitate the immune system to simulate a systemic infection, to persuade it that the enemy it is being shown is really dangerous. This persuades the immune system to rush off and make loads of antibodies which can take out the offending cut up sections of the enemy protein, the spike protein, for Covid vaccines.
The purpose of the above mini course in basic immunology is to educate the reader to the point where they understand that vaccines cannot lose effectiveness. Vaccines are DIGITAL. They are not ANALOGUE. They offer a 2-3 week training course to the immune system which either works or does not work. After that they have nothing whatsoever to do. They carry out no further process which can lose efficiency. Either they show the immune system part of the virus and alert it to the danger it poses or they do not. We know that the covid19 vaccines work initially, from the initial case number results. So they succeed in training the immune system. At the point their job is done. They have nothing more to do. There is no immunological mechanism by which vaccines can lose their efficiency because they have finished the purpose of their existence within 2-3 weeks, the normal period of a viral infection. The concept that they lose efficiency after 2-3 weeks is just immunological nonsense.
So the rapid deterioration in immune response to Covid19 post vaccination can only be due to the vaccines damaging the immune system. It cannot be due to them ‘losing efficiency’. The fact that the boosters do improve covid response (by alerting the immune system even more and telling it that covid19 – which has already been identified twice by the first two shots, is really really really dangerous and it had better go to defcon3) shows categorically that vaccines have not lost their efficacy. Their training program is still effective. So the deterioration in immune response is an unwanted side effect of the vaccination. It is the gene therapy part of the vaccines. It is the continual over production of spike proteins that appears to wear out the poor old immune system. And boosters will make that worse.
Further Government Covid Data Manipulation
The ONS published deaths from all causes by vaccination status in excel format https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/datasets/deathsbyvaccinationstatusengland
We combine their tables 4 and 5 as below. Their data covers the period from Janaury8 to September24. It includes 10-17 year olds in the unvaxxed group. these could not be vaccinated prior to August23. So one needs to remove them and further one needs to find a way to adjust the data for their dependency upon age because vaccinated people are generally older that unvaccinated people. The ONS does this with their Age Standardised Mortality Rate formula. https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/methodologies/weeklycovid19agestandardisedmortalityratesbyvaccinationstatusenglandmethodology
They use this to provide ‘Age Adjusted’ figures. they do this because the fact is that every single week from late January to September24 the rate of death among the vaccinated has far exceeded that rate among the unvaxxed. Even when we remove the 10-17 year olds as we have done in the table below (we calculated below that there are 4,434,375 of them in the ONS invaxxed group), it is still the case that for most of May you were 5x more likely to die if you were in the vaccinated group than if you were in the unvaccinated group.
Admittedly, even with the 10-17 year olds removed the vaccinated group was still considerably older than the unvaxxed group in May. But this is not the sort of thing the government want to be publishing. So they try to shift your focus to their ‘Age adjusted’ figures, which they call their ‘Age standardised’ figures because that sounds less manipulative. But here is the raw data with the teenagers removed…

The ONS in their Table 4 and Table 5 calculated the death rates per 100k using the complicated age standardised mortality rate formula explained in their report. This is supposed to remove age as a confounding factor in the table above. The main confounding component is the inclusion of death rates for 10-17 year olds in the unvaccinated group during a period when nobody under 18 could become vaccinated. The obvious method of fixing that disparity would be for the ONS to simply remove people whose age was less than 18 from the group. But they chose instead to leave them in and then take them back out again with a complicated formula as bureaucrats love to do.
However we can see how many 10-17 year olds there were in the ONS unvaxxed group on 20-Aug-21 (16-17 year olds were called to be vaccinated on 23-August-21) as follows.
UK 10-17 = 5,305,102 (ONS mid year population estimates June2020)
UK population 10+ = 49,771,233 (ONS mid year population estimates June2020)
On 23-Aug-21 –
UK singly vaxxed = 39,910,686 (https://coronavirus.data.gov.uk/details/vaccinations)
UK unvaxxed 10+ = 9,860,547
ONS unvaxxed = 8,242,156
Ratio ONS/UK = 83.587%
83.587% of 5,305,102 = 4,434,375
So we should have 4,434,375 10-17s to remove. We took that number from the 10+ unvaxxed population column above to calculate the 18+ column.
Having removed the teenagers we can see where the death rate will be when age has worked its way out of the data (by October22 when everyone over 18 who wanted a second shot has had 10 weeks in which to get one given their call for the 1st shot was June18 and there should be an 8 week gap between shots. So their call for the 2nd shot was August13).
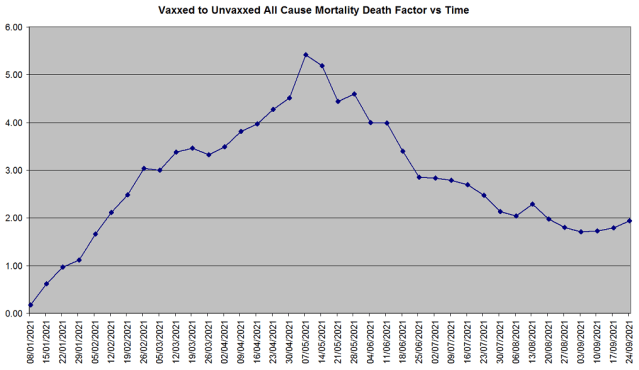
The Death Factor is simply the ratio of the Vaccinated all cause death rate per 100k to the Unvaccinated
All death rates per 100k are calculated by multiplying the number of deaths by 100,000 and dividing them by the population of the group
If we go forward by 5 weeks from September24 to October29 we reach the time when everybody 18 and over has had the opportunity to get vaccinated if they want it. So the age disparity between the vaccinated and the unvaccinated will have settled down. The graph above shows that the final position will be that the death rate in the vaccinated people will be TWICE the death rate in unvaccinated people TODAY.
Even that 2:1 ratio is affected by age because younger fitter more athletic and sporty people and people with faith in God or in nature, do not feel the need to take the vaccine because they trust their own bodies and nature or God more than they trust massive profit driven government lobbying Pharmaceutical companies.
However the ONS does not mention this 2:1 final ratio of all cause mortality rates in the vaxxed compared to the unvaxxed in their monolateral pro gene therapy Bulletins. Instead they tell us the following in their latest bureaucratic extravaganza of age standardisation…

This does not plot true death rates by vaccination stauts against time. It plots Age Standardised Mortality Rate by vaccination status against time.
So the UKHSA says that unvaxxed people are dying of Covid at 5x the rate of the doubly vaxxed due to their age standardisation mortality rate formula. Whereas the raw figures for the week to September24 show that the unvaxxed are only dying at twice the rate of the doubly vaxxed (2.97:1.5) from Covid. Furthermore the doubly vaxxed are dying of all causes at twice the rate of the unvaxxed ! So we must look at the UKHSA Age Standardised Mortality Rates for all causes for the last 10 weeks. Here they are from Table2.

These are saying the the doubly vaxxed have had on average a true non age biased death rate which is 58% of the unvaxxed death rate from all causes. If that analysis had any bearing on reality at all, then since the doubly vaxxed (who make up the vast majority of the population) would be dying at 58% of the rate of the unvaxxed, all cause mortality for the entire population would be close to 58% of the 5 year average. Because unvaxxed people at present are not dying in significant numbers from Covid and have had no medical intervention. So they would represent the 5 year all cause mortality rate. Well here is the present all cause mortality rate for the entire country…https://www.ons.gov.uk/peoplepopulationandcommunity/birthsdeathsandmarriages/deaths/bulletins/deathsregisteredweeklyinenglandandwalesprovisional/22october2021

All Cause Mortality has not dropped to 58% of the 5 year average. No. It has risen to be around 15% greater than that average. The Age Standardised Mortality Rate produces a work of bureaucratic fiction by a factor of around 2 – so desperate are the government to cover up the true picture for Covid, which is that the vaccinated are presently raising all cause mortality in the UK by 15%. And since they make up 80% of the population, their true age independent death rate will need to be 19% above that of the unvaxxed in order to achieve that.
What this means is that for every person the vaccines are saving from covid, they are killing 1.19 people from side effects.
Last year at this time all cause mortality was also elevated above the 5 year average due to significant numbers of covid deaths from Wuhan alhpa. This year we have just as many cases, but many fewer deaths, thank God. Because delta, although more infectious, is less lethal. So the elevation is not due to delta. It must be due to the vaccines.
In conclusion: The ASMR formula is biased in favour of the doubly vaxxed and against the unvaxxed by a factor of 2.
What this means is that the true Covid death rate among the vaccinated is no better than among the unvaccinated, which is the inescapable immunological conclusion from the fact that case rates are higher in the vaccinated. For death rates should follow case rates.
_______________________________
If you are looking for solutions (lawyer, form, gathering, action, maybe this could help you:
HERE
If you like our work please consider to donate :

Related posts:
Views: 0
 Posted in
Posted in  Tags:
Tags: 
















