 RSS Feed
RSS Feed

















 August 8th, 2017
August 8th, 2017  Awake Goy
Awake Goy 
On August 2, 2017, The Nation published an article by Joshua Holland, “Medicare for All isn’t the Solution for Universal Health Care,” chastising Improved Medicare for All supporters because, in his view, the single payer movement has “failed to grapple with the difficulties of transitioning to a single-payer system.” The article, which doesn’t quote anyone involved in the movement for Improved Medicare for All, begs a response because it shows what liberals opposed to single payer believe. Holland dredges up the same arguments used to keep single payer off the table during the creation of the Affordable Care Act (ACA). He even dusted off a few that were used to try to stop Medicare from coming into existence in the 1960s. And then he attempts to distract single payer supporters away from supporting Improved Medicare for All and settling for something less, as was done successfully in 2009.
The first error that Holland makes is confusing the term “Medicare for All” as meaning that advocates would simply take the current Medicare system, with both traditional and ‘Advantage’ plans, and expand that. This is why it is important to use the phrase “Improved Medicare for All.” As outlined in HR 676: The Expanded and Improved Medicare for All Act, the new system would be based on the current Medicare system, which is already national, but it would be a single public plan that is comprehensive in coverage and does not have out-of-pocket costs or caps. It would ban investor-owned facilities and ban private insurers from selling policies that duplicate what the system covers. A single system is the simplest for patients and health professionals because there is one transparent set of rules.
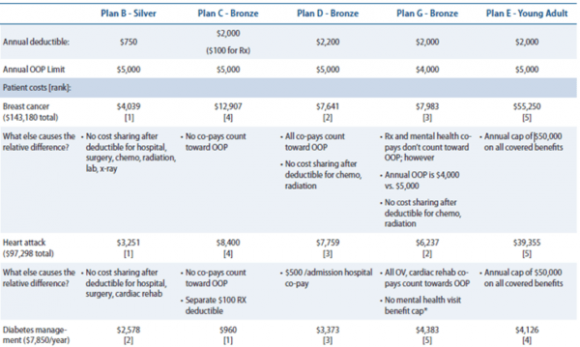
Most people who purchase health insurance have no idea which plan is best for them because nobody can anticipate what their healthcare needs will be in the future. A study of the Massachusetts health exchange plans done by the Center for American Progress showed that some plans were best for patients with cancer and other plans were best for people with heart disease or diabetes, but that isn’t something that can be advertised up front. Even if it were, people can’t predict if they will be diagnosed with cancer, heart disease or diabetes in the future. HR 676: The Expanded and Improved Medicare for All Act solves this problem by creating a single public plan designed to cover whatever our healthcare needs will be.
A second error that Holland makes is saying that HR 676 calls for the new system to start within a single year. The bill will take effect “on the first day of the first year that begins more than [emphasis added]1 year after the date of the enactment of this Act.” This means that if HR 676 were to be signed by the President in July of 2018, then it would take effect in January of 2020. Holland raises the concern that we can’t move the whole country into the new Improved Medicare for All system that quickly. In fact, HR 676 has transition periods for the Veteran’s Administration, the Indian Health Service, displaced workers and buying out for-profit health providers.
When Medicare was enacted in 1965, more than 50% of seniors were uninsured and the rest had some form of health insurance. Without computers and without a national health system in place, all 19 million seniors were enrolled in the first year (almost twice as many as were enrolled in the ACA in the first four years). At present, the United States has Medicare infrastructure in place and all practicing health professionals have a National Provider Identifier issued to them by the Centers for Medicare and Medicaid Services (CMS). When the new Improved Medicare for All system takes effect, enrollment will be very simple because there is only one plan that is universal and paid for up front though taxes. All health professionals will be in it. Every person could be sent a card, much as CMS does now for people who are turning 65. For those who do not receive a card, HR 676 has a solution – when they present for care at a health facility, they are assumed to be in the system, are treated first and then are enrolled in the system afterwards.
Next, Holland brings up the same arguments used to prevent universal health care attempts in the past. He states that people don’t want to give up what they have. This is called ‘loss aversion.’ It is a task of the single payer movement to build the public support for Improved Medicare for All necessary to overcome any potential loss aversion. Public figures and elected officials can play a role in building support as well.
Holland raises concerns that employers and seniors won’t want to give up their private plans, but that is based on his mistaken belief that Improved Medicare for All will be the same as current Medicare. The reality is that people will be less worried about giving up what they have if they know that it will be replaced with something better and that they will no longer fear losing their doctor as they will all be in the new system. Improved Medicare for All will provide more comprehensive benefits, no out-of-pocket costs and an unrestricted network of health professionals from which to choose. Employers will no longer be burdened with the high costs of health insurance. People with pre-existing health conditions will no longer worry about losing coverage or having to pay more. Unions and employers can offer supplemental plans for extras not covered by the new system, as is done in countries like France, if they choose to do so.
Holland also raises the concern that people will lose their doctor because they will opt out of the system due to low reimbursements. We are already losing doctors because of the current system. Physician burnout was listed as the second biggest concern by the Surgeon General last year. Under Improved Medicare for All, all health professionals will be in the system. There won’t be any place to opt out to. And why would they want to? Health professionals will save tens of thousands of dollars each year on billing and won’t have to worry about whether a patient has insurance or not. They can see anyone who calls for an appointment. And they will have a system with which to negotiate fair reimbursement. Private health insurance doesn’t negotiate with physicians and hospitals. Each year they make an offer and providers can either basically take it or leave it. Doctors in single payer systems that spend much less per capita than the United States are paid well, so the US can certainly afford to reimburse doctors adequately.
 Every transformative change has suffered from loss aversion, but that hasn’t stopped them. When Medicare was enacted, it was called socialized medicine, a government intrusion that would take away people’s choices and freedom and become an opening to government control over our lives. The scare tactics didn’t work and Medicare is one of the most popular parts of our current healthcare system. Desegregation, women’s rights, workers’ rights and more were great changes that were successful and we are a better society for them. Why is the right to health care any different?
Every transformative change has suffered from loss aversion, but that hasn’t stopped them. When Medicare was enacted, it was called socialized medicine, a government intrusion that would take away people’s choices and freedom and become an opening to government control over our lives. The scare tactics didn’t work and Medicare is one of the most popular parts of our current healthcare system. Desegregation, women’s rights, workers’ rights and more were great changes that were successful and we are a better society for them. Why is the right to health care any different?
Finally, Holland dives into the myth that we can’t afford Improved Medicare for All because it will be too expensive. My first response when I hear this is that the same excuse wasn’t made when we spent $16 trillion to bail out the banks in 2008 and is never made when we invade another country, so why is it raised when it comes to one of the most basic necessities a society can have? The United States has the highest wealth and the highest wealth inequality of industrialized nations. The new “Commitment to Reducing Inequality Index” recommends social spending on education, health and other basic social protections as its top priority. Congress can appropriate the funds to do this. This should be a top priority in the United States as well.
The reality is that the United States is already spending the most on health care per person each year because the market has failed to control costs. That is exactly why we need a single payer system like National Improved Medicare for All. It is the only way to simplify the bloated bureaucracy of the current healthcare system, which would save around $500 billion each year, and to control the costs of medical procedures, medical devices and pharmaceuticals by having a single system that can negotiate fair prices. In addition to the bureaucracy created by a multi-payer system, the US subsidized the insurance industry with more than $300 billion last year. A system based on health, rather than profits for investors, can identify and prioritize our greatest health needs and work to address them.
For example, the US is failing when it comes to care for people with chronic diseases. There are numerous reasons why this is occurring – lack of access to consistent care, inability to afford medications, insufficient time for health education when patients see a health professional, cheap and highly processed food, environmental pollutants and more. An actual health system could take meaningful action to address these issues, and keep people healthier. Think about it: people with high blood pressure or diabetes in the US may not be able to see the doctor regularly or stay on their medicines due to cost, but when they suffer a stroke or kidney failure, and need long term care or dialysis, then they can receive disability benefits and Medicare. How much better and less expensive would it be for everyone to prevent strokes and kidney failure in the first place?
Just as many ‘progressive’ groups did during the health reform process that resulted in the ACA, Holland works to convince us that we don’t need a single payer system, and that we can work with the current system. Once again, Jacob Hacker, a leading advocate for the ACA and single payer opponent, is invoked and we are told that we can add a Medicare buy-in or another form of a public option. We are told that other countries use private insurance, so why can’t we? The Democrats, beholden to the medical industrial complex, want us to believe these false non-solutions that protect the insurance industry. It feels like 2009 all over again.
Rather than go through all of the reasons why these approaches will fail, I urge you to read articles on that topic posted on HealthOverProfit.org (Click here for a list of them). Instead, I refer to a saying used by my now-deceased mentor Dr. Quentin Young: “You can’t cross an abyss in two jumps.” The only way we can get to a universal single payer healthcare system in the United States is by creating a universal single payer healthcare system in the United States. Anything less than that will fail because it will not achieve the savings on administration and prices needed to cover everyone and it will not compete with the powerful private insurance industry.
Throughout time, every great social movement has been told that it was asking for too much. Advocates for worker’s rights, women’s rights, civil rights, etc., were labelled as unreasonable radicals wishing for some pie-in-the-sky change that can’t be achieved. Holland is doing the same to the single payer movement. Don’t fall for it. We have the resources in the US to have one of the top healthcare systems in the world. We have health policy experts who have helped to design excellent systems for other countries. Single payer is a proven solution, unlike the plans being proposed by the Democratic leadership.
One thing that Holland and I do agree on is that there is more than one way to skin a cat, so to speak. We could have an excellent national debate about which type of single payer healthcare system we support – a fully socialized system like the Veteran’s Health Administration, a national health service, or a socialized payer with multiple types of providers as in the Expanded and Improved Medicare for all Act. At the basis of our discussion must be the principles that every person in the US deserves high quality health care without financial barriers.
Source Article from https://popularresistance.org/response-to-the-nation-improved-medicare-for-all-is-the-solution/
Related posts:
Views: 0
 Posted in
Posted in  Tags:
Tags: 
















