 RSS Feed
RSS Feed

















 May 14th, 2017
May 14th, 2017  Awake Goy
Awake Goy To question public vaccine policy is to commit the crime of heresy against the vaccine religion, as illustrated by how any dissent is met by its defenders.
There is something wrong when you are not allowed to question public vaccine policy without automatically being labeled as “anti-science”, a believer in “pseudoscience”, or even a “conspiracy theorist”. The subject of vaccines is a serious one, and deserves to be taken seriously. Concerned parents are asking legitimate questions, and they deserve serious answers rather than dismissals. The public discussion about vaccines is essentially non-existent. Instead, the message we are told is that there is nothing to discuss. The mainstream media, for its part, has utterly failed to properly inform the public about the subject of vaccines, and rather than engaging in respectful debate, there is a tendency to try to bully people into silence and compliance. In this endeavor, the mainstream media has useful partners in the blogosphere.
As someone who is openly critical of vaccine policy, I expect to be attacked and have such labels mindlessly flung at me. So I wasn’t surprised to discover that one of the more notorious apologists for public vaccine policy, an anonymous blogger who goes by the moniker “Skeptical Raptor“, set his sights on me recently for an article I wrote in response to a Washington Post op-ed by Dr. Daniel Summers. Dr. Summers took the usual dogmatic approach to the subject, insisting there is nothing to debate, just get your damned shots. The purpose of my rejoinder to his op-ed was to illustrate why this insistence is wrong. There is a discussion to be had about vaccines, and it’s past time we started having it.
Raptor’s response to that article of mine provides me with the opportunity to reiterate that same point, as well as to illuminate the kinds of tactics employed by those who try to intimidate into silence anyone who dares to question public vaccine policy — rather than seriously addressing the legitimate concerns being raised.
Naturally, Raptor’s post about my article is filled with such mindless attacks as:
- “Jeremy R. Hammond … attacked Dr. Summers with … tropes, myths, and conspiracy theories.”
- “Hammond uses pseudoscience….”
- “Hammond’s criticisms of Dr. Simmons [consist of] tropes, myths, conspiracy theories, cherry picking and, need I mention this, outright misinformation.”
- “But if you want to believe the ramblings of a right wing science denier, go right ahead.”
It’s instructive, given such vitriolic rhetoric, that Raptor fails to point to even a single error in fact or logic in anything I wrote in my rejoinder to Dr. Summers. (Which might explain why Raptor didn’t link to my article so readers could check to see for themselves what I’d actually written, as opposed to his misportrayal.)
On Doctors’ Confirmation Bias
In my article, I quoted Dr. Summers saying that if vaccines can cause autism, then pediatricians like him must either be “too incompetent to discern the relationship between the two” or “too monstrous to care”.
I observed that this gives us a useful insight into why doctors might easily succumb to confirmation bias, accepting of science that confirms their belief that they are competent and good while dismissing any evidence contradicting that belief. After all, how many doctors would be honest enough to admit that they are either incompetent or evil?
So how does Raptor respond to this observation? He writes:
First of all, Hammond does not quite understand confirmation bias. In fact, most of us who support vaccines use the scientific method – the evidence leads us to a conclusion. Hammond uses pseudoscience – establish a conclusion, like vaccines cause autism, and ignore all evidence that does not support his beliefs…. Frankly, Hammond is projecting the problems with his own arguments onto Dr. Simmons.
In other words, Raptor is saying that I’m the one guilty of confirmation bias, and that I don’t understand what confirmation bias is. So what is confirmation bias? Here’s how Raptor defines it:
[C]onfirmation bias is simply the tendency for individuals to favor information or data that support their beliefs. It is also the tendency for people to only seek out information that supports their a priori, or pre-existing, conclusions, and subsequently ignores evidence that might refute that pre-existing conclusion.
I’m perfectly content to use that definition to reiterate the point I made in my response to Summers: that doctors will tend to have a confirmation bias because it would be difficult for them to accept that something they did to a child with the intention of helping that child might have ended up harming that child.
Note that Raptor does not actually address this point. He simply asserts that I don’t understand confirmation bias without bothering to demonstrate in what way I don’t understand it and meaninglessly declares that doctors “use the scientific method” — as though having a medical degree meant that a person couldn’t possibly have such a psychological conflict.
Compare this with Dr. Joseph Mercola of the leading health information website Mercola.com, a physician who once vaccinated his patients and had to overcome this very inner conflict himself; Dr. Mercola in a recent article on his website quoted my observation about this natural tendency toward confirmation bias among doctors, then added:
As a doctor, I can empathize with this psychological conundrum. It’s a terrible feeling to realize that, at some point in your life, you didn’t have the knowledge you should have had and you led your patients the wrong way.
In conclusion, Raptor, rather than actually addressing my valid point, resorts to obfuscation.
As for his charge that I’m guilty of confirmation bias, here Raptor is simply resorting to strawman argumentation, attributing to me logic that I did not use in my response to Summers’ op-ed. His protest against what I did say in my article on the subject of vaccines and autism is instructive.
The Autism Question
In my article, I criticized Dr. Summers for repeating the trope that the hypothesis that vaccines can cause autism has been “thoroughly debunked”. I pointed out that the government has in fact acknowledged that vaccines can cause brain damage in genetically susceptible individuals, and that this brain damage can lead to developmental regression, i.e., autism. I quoted then Director of the CDC Julie Gerberding in 2008 admitting:
Now, we all know that vaccines can occasionally cause fevers in kids. So if a child was immunized, got a fever, had other complications from the vaccines. And if you’re predisposed with a mitochondrial disorder, it can certainly set off some damage. Some of the symptoms can be symptoms that have characteristics of autism.
Then I commented: “So seems to me there’s some room for debate there. (Gerberding, incidentally, left her government job to become head of Merck’s vaccine division.)”
So how does Raptor respond to this point? Raptor simply asserts that “there are hundreds of studies that have debunked Hammond’s belief.”
But what “belief” of mine is Raptor referring to, exactly? Are there hundreds of studies that have “debunked” that the head of the CDC acknowledged vaccines can cause brain damage leading to developmental regression? Or does Raptor mean hundreds of studies have “debunked” what Gerberding said?
Is this former CDC director and president of Merck’s vaccine division into “pseudoscience”?
We see once again all Raptor is doing is attempting to obfuscate the point. Raptor continues this effort by writing:
Next, Hammond claims that the “government has actually acknowledged that vaccines can cause brain damage, and that this vaccine-caused brain damage can result in developmental regression in genetically susceptible individuals.”
The “Next” here is puzzling, since this point about the head of the CDC acknowledging vaccines can cause brain damage was the one and only point I made in response to Dr. Summer’s repetition of the usual dogmatic mantra about any association having been “debunked”.
Setting that aside, note how Raptor uses the verb “claims” — as though it wasn’t a fact that the CDC director acknowledged that vaccines can cause brain damage leading to developmental regression. This verb choice is puzzling, given how Raptor then proceeds to share the statement of Gerberding’s that I quoted.
So how does Raptor address my point about that acknowledgment from the CDC director? Raptor writes:
Sure, that’s an admission that vaccines can cause brain damage – in a child with an extremely rare disorder.
Note that Raptor acknowledges that vaccines can cause brain damage in genetically susceptible individuals.
Raptor nevertheless continues:
Hammond, in the purest sense of pseudoscience, grasps onto a very rare adverse effect, and uses it to “prove” vaccines cause autism. It most certainly does not.
Now, this is also quite a puzzling argument, given the actual context of the quote from Gerberding.
See, when she spoke those words, the CDC director was referring to the case of Hannah Poling, who developmentally regressed and was diagnosed with autism after receiving five vaccines at once at 19 months of age.
Inspiration and all our best content, straight to your inbox.
The Poling Case and Genetic Susceptibility
One of the legitimate concerns parents have about vaccines is how the government constantly reassures them that vaccines are safe and effective while granting legal immunity to the vaccine manufacturers, which was upheld by the Supreme Court on the grounds that injuries from vaccines are “unavoidable”. Under the 1986 law granting this legal immunity, the National Vaccine Injury Compensation Program (VICP) was set up to shift the cost burden from vaccine injuries away from the pharmaceutical industry and onto the taxpayers.
Naturally, parents are confused by this, and it certainly raises some legitimate questions.
The Poling family is among those who have been awarded compensation under the VICP. In the case of Hannah Poling, the government acknowledged that:
The facts of this case meet the statutory criteria for demonstrating that the vaccinations CHILD received on July 19, 2000, significantly aggravated an underlying mitochondrial disorder, which predisposed her to deficits in cellular energy metabolism, and manifested as a regressive encephalopathy with features of autism spectrum disorder.
Now given the context of Gerberding’s admission, note what Raptor is effectively arguing: the fact that vaccines can cause brain damage resulting in autism doesn’t prove that vaccines can cause autism!
One could also argue that the fact you ran over a nail with your bicycle doesn’t prove that the nail caused your flat tire — technically, it was the hole in the tire that did it.
Scientific American has commented on the Poling case by saying that “Theoretically, that makes sense” (that the vaccines triggered the cascade of events resulting in her autism). In Hannah’s case, her mitochondria, the “power plants of the cell”, were “already underperforming, so when she developed a fever from her vaccine, the increased energy requirements likely pushed them past their thresholds”, triggering her autism symptoms.
Evidently, Scientific American is into “pseudoscience”, too.
Another propagator of “pseudoscience” was Bernadine Healy, M.D., former director of the National Institutes of Health and president and CEO of the American Red Cross. Before her death, she had come to challenge the official dogma, writing that as a trigger of autism, “vaccines carry a ring of both historical and biological plausibility”.
But what about all those studies Raptor mentions that supposedly have proven there is no possible causal association between vaccines and autism?
As Healy also said in an interview, “I think that the public health officials have been too quick to dismiss the hypothesis as irrational.”
When her interviewer pointed out that public health officials had been saying that “there’s enough evidence and they know its not causal”, Healy’s response was, “I think you can’t say that. You can’t say that.”
Healy then offered another explanation for how confirmation bias can become institutionalized:
There is a completely expressed concern that they don’t want to pursue a hypothesis because that hypothesis could be damaging to the public health community at large by scaring people.
Healy also noted the lack of studies into — and lack of interest in studying — the possibility of some individuals having a genetic susceptibility to vaccine injury:
If you turn your back on the notion that there is a susceptible group… what can I say?
Hannah Poling’s father, Jon Poling, who happens to be a neurologist, has made the same observation about both the institutional confirmation bias and the lack of studies examining the question of whether vaccines can cause autism in genetically susceptible children:
With regard to the science of Autism, I have no argument with the assertion that a single case does not prove causation of a generalized autism-vaccine link. What the case does illustrate though is a more subtle point that many physicians cannot or do not want to comprehend (ostensibly because vaccines are too important to even question). Autism is a heterogeneous disorder defined by behavioral criteria and having multiple causes. Epidemiological studies which have not found a link between autism and aspects of vaccination do not consider the concept of autism subgroups. Indeed, in a heterogeneous disorder like Autism, subgroups may indeed be ‘vaccine-injured’ but the effect is diluted out in the larger population (improperly powered study due to inability to calculate effect size with unknown susceptible subpopulation). I think former NIH Director, Dr. Bernadine Healey explained it best in that population epidemiology studies are not “granular” enough to rule-out a susceptible subgroup.
Then there’s Dr. Frank DeStefano, who has acknowledged that “it’s a possibility” that vaccines could trigger autism in genetically susceptible individuals.
Evidently, this CDC Director of Immunization Safety, who has coauthored several of the CDC’s studies finding no link between vaccines and autism, is into “pseudoscience”, as well.
The trouble is, DeStefano added, “It’s hard to predict who those children might be”, and trying to determine what underling conditions put children at risk of vaccine injury is “very difficult to do”.
Acknowledging the lack of studies in this area, he added that, “if we ever get to that point, then that kind of research might be fruitful.”
And here’s the CDC’s website, current as of this writing, on the lack of such studies: “More research is needed to determine if there are rare cases where underlying mitochondrial disorders are triggered by anything related to vaccines.”
When I contacted the industry-funded American Academy of Pediatrics (AAP) recently to request them to provide studies that considered the existence of genetically susceptible subpopulations to support their claim that any association between vaccines and autism had been “disproven”, the AAP provided me with a list of studies. Not one of the studies provided by the AAP considered the possibility of a genetically susceptible subpopulation.
I pointed this out to the AAP, and I also pointed out that it isn’t logically possible to say — as they had in their press release — that a hypothesis has been “disproven” when it hasn’t even been studied. I therefore then once more asked whether they could produce any studies that considered the existence of genetically susceptible individuals. The AAP’s response was that they had already provided all that they were going to provide.
When I asked whether the authors of the press release would like to comment, I was told by the AAP representative that she was going to hang up on me, which she promptly did.
Now, for good measure, let’s turn to the medical literature on this question and look at a couple of papers written by individuals who can by no means be labelled “anti-vaxxers” to see what they have to say about the hypothesis that vaccines can cause autism in children who are genetically susceptible to vaccine injury.
Dr. Paul Offit and ‘Poor Reasoning’
In a September 2008 paper in the journal Paediatrics & Child Health, Asif Doja argues against a causal relationship between vaccines and autism, yet acknowledges that “Mitochondrial disorders represent a rare cause of autism” — as well as the possibility that vaccines could cause fevers that in turn could cause encephalopathy (brain damage) and regression in individuals with mitochondrial dysfunction.
Doja is careful to emphasize that it is the fever that causes the encephalopathy, “not the vaccine itself”. (It was the hole in the tire that caused it to go flat, not the nail, remember.)
Doja also argues that “it is unlikely that those with mitochondrial disease simply require a vaccine ‘trigger’ to set off the disease process because most patients with mitochondrial disease do not have an onset of symptoms associated with vaccination.”
But this argument is a logical fallacy. It’s a non sequitur; the conclusion doesn’t follow from the premise. It may be true that most patients with mitochondrial disease do not have an onset of symptoms associated with vaccination, but it does not follow that it is therefore “unlikely” that vaccines could be the necessary “trigger” in some children.
The title of Doja’s article, “Genetics and the myth of vaccine encephalopathy”, is a curious one, given how, despite his fallacious conclusion that it’s “unlikely”, Doja ultimately acknowledges the possibility that “fever associated with the vaccine” could provoke “the initial seizure” ultimately resulting in brain damage in genetically susceptible individuals.
Doja also cites another article, published in the New England Journal of Medicine, by Dr. Paul Offit. So let’s look at that one, as well.
Paul Offit is someone whose credentials as a defender of public vaccine policy are impeccable.
He was sitting on an advisory board for the vaccine manufacturer Merck at the time he wrote that article.
Offit is also a former member of the CDC’s vaccine advisory committee, a body that helps determine public vaccine policy. As a member of that committee, Offit advocated that the CDC recommend use of the rotavirus vaccine. He later profited handsomely from the sale of a patent for a rotavirus vaccine.
Offit has made insane claims and is unafraid to brazenly lie knowing that, given the current climate surrounding the vaccine issue, his colleagues in the medical establishment will not hold him accountable for it. For instance, he is famous for once claiming that children could safely handle 10,000 vaccines at once. Another time, he declared that “Aluminum is considered to be an essential metal with quantities fluctuating naturally during normal cellular activity. It is found in all tissues and is also believed to play an important role in the development of a healthy fetus.”
Offit is the director of the so-called “Vaccine Education Center” at the Children’s Hospital of Philadelphia, where he also holds the Maurice R. Hilleman Chair in Vaccinology, created in honor of the former senior vice president of Merck, which provided a $1.5 million endowment to “accelerate the pace of vaccine research”.
Offit also happens to be the mainstream media’s go-to guy when a comment is needed on anything related to vaccine safety. When you read an article in the mainstream media about vaccines, there’s a pretty good chance you’ll find a quote from Offit in it (which says a lot about mainstream journalism). He’s been appropriately dubbed by Philadelphia magazine as “Mr. Vaccine”.
In the New England Journal of Medicine, Offit describes what happened to Hannah Poling:
When she was 19 months old, Hannah, the daughter of Jon and Terry Poling, received five vaccines — diphtheria–tetanus–acellular pertussis, Haemophilus influenzae type b (Hib), measles–mumps–rubella (MMR), varicella, and inactivated polio. At the time, Hannah was interactive, playful, and communicative. Two days later, she was lethargic, irritable, and febrile. Ten days after vaccination, she developed a rash consistent with vaccine-induced varicella.
Months later, with delays in neurologic and psychological development, Hannah was diagnosed with encephalopathy caused by a mitochondrial enzyme deficit. Hannah’s signs included problems with language, communication, and behavior — all features of autism spectrum disorder….
For years, federal health agencies and professional organizations had reassured the public that vaccines didn’t cause autism. Now, with DHHS making this concession in a federal claims court, the government appeared to be saying exactly the opposite.
Offit goes on to argue that the government’s decision was “poorly reasoned”.
His first argument is that, while “it is clear that natural infections can exacerbate symptoms of encephalopathy in patients with mitochondrial enzyme deficiencies, no clear evidence exists that vaccines cause similar exacerbations.”
Compare this denial of Offit’s to Doja’s acknowledgment in his Paediatrics & Child Health article that “indeed febrile seizures have been shown to occur at an increased rate after vaccination”.
Seizures are a recognized symptom of encephalopathy.
In fact, Offit himself just two paragraphs later acknowledges that “experts testifying on behalf of the Polings could reasonably argue that development of fever and a varicella-vaccine rash after the administration of nine vaccines was enough to stress a child with mitochondrial enzyme deficiency” (emphasis added).
Offit’s second argument is that due to technological advancements, the combined schedule of fourteen vaccines children received in 2008 (the time of his writing) exposed children to fewer “immunologic components” than just the one smallpox vaccine from a century ago, “which contained about 200 structural and nonstructural viral proteins”.
This argument, however, overlooks, among other things, that the immunologic components of the target antigen (i.e, the virus or bacteria the vaccine is designed to prevent the disease of) are not the only antigens contained in vaccines.
The smallpox vaccine did not contain aluminum or mercury, for example, both known neurotoxins contained in CDC-recommended vaccines today. (Aluminum is used as an adjuvant in some vaccines to cause a stronger immune response than the target antigen would alone, and influenza vaccines that come in multi-dose vials still contain the preservative Thimerosal, which is 50 percent ethylmercury by weight. Other vaccines may contain “trace amounts” of mercury from the manufacturing process.)
As another example, vaccines can also contain contaminants, such as retroviruses. This is not theoretical; numerous vaccines have been found to be contaminated with other viruses or viral fragments. Polio vaccines used in the late 1950s and early 1960s, for example, were contaminated with a monkey virus (simian virus 40, or SV40) that’s been associated with an increased risk of some cancers.
In fact, the vaccine Offit himself helped develop, Merck’s Rotateq, was found to be contaminated with pig virus DNA. GlaxoSmithKline’s rotavirus vaccine, Rotarix, was suspended from the market in 2010 because it was found to be contaminated with a pig virus.
Offit’s third argument is that “Hannah had other immunologic challenges that were not related to vaccines”; namely fevers and ear infections. “Children typically have four to six febrile illnesses each year during their first few years of life; vaccines are a minuscule contributor to this antigenic challenge.”
Offit’s logic here rests essentially on the same fallacy as Doja’s: it does not follow from the fact that most fevers in children are not caused by vaccinations that therefore it can’t be that, in some cases, vaccines are the trigger that sets off the cascade of events leading to developmental regression.
Offit further argues that Hannah’s autism was caused by her mitochondrial disorder, not the vaccines she received.
This is like arguing that celiac disease is caused by a patient’s HLA-DQ2 and HLA-DQ8 genes, not by gluten consumption. Just as having the genetic predisposition “is necessary for disease development but is not sufficient for [celiac] disease development” (Genomic Medicine), so it is that having a mitochondrial disorder does not necessarily mean that the child will develop autism; one or more environmental triggers are also required.
Amidst his protests against the conclusion that the vaccines Hannah received caused her autism, Offit nevertheless acknowledges the “theoretical risk” of “exacerbations” from vaccines in children with mitochondrial disorders andthe absence of “data that clearly exonerates vaccines” in this respect.
As Hannah’s father, Jon Poling, and three co-authors wrote in a case study published in the Journal of Child Neurology,
It is unclear whether mitochondrial dysfunction results from a primary genetic abnormality, atypical development of essential metabolic pathways, or secondary inhibition of oxidative phosphorylation by other factors. If such dysfunction is present at the time of infections and immunizations in young children, the added oxidative stresses from immune activation on cellular energy metabolism are likely to be especially critical for the central nervous system, which is highly dependent on mitochondrial function. Young children who have dysfunctional cellular energy metabolism therefore might be more prone to undergo autistic regression between 18 and 30 months of age if they also have infections or immunizations at the same time.
Now recall Raptor’s admission “that vaccines can cause brain damage – in a child with an extremely rare disorder”. In other words, despite his best efforts to obfuscate my point, Raptor tacitly acknowledges that what I wrote is true.
On ‘the cancer-preventing HPV vaccine’
Another statement I quoted from Dr. Summers’ Washington Post op-ed was:
Despite ample evidence of its safety and efficacy, many parents choose not to give their children the vaccination against the carcinogenic human papillomavirus, leaving their sons and daughters at increased risk of several different cancers.
In response, I wrote:
Can Dr. Summers point to any studies in the medical literature that have shown that the HPV vaccine reduces the risk of developing cervical cancer (or anal or mouth/throat cancers in men)? When the FDA approved its use allowing the vaccine manufacturers to advertise it on the grounds that it can prevent cancer, had this been proven in clinical trials?
The answer to both questions is “No”. Dr. Summers’ assertion is an assumption, not a demonstrated fact. Room for debate on that one, too, then.
Raptor writes that here I am “relying upon all of the tenets of pseudoscience and science denialism” to “trash Gardasil” (Merck’s HPV vaccine).
Raptor then declares that he “can point to several” studies in the medical literature that have shown that the HPV vaccine reduces the risk of cervical cancer. In an attempt to support this claim, Raptor then provides five links. Turning to Raptor’s very first source cited, we find a study published in the Journal of the National Cancer Institute.
Does this study show that the HPV vaccine reduces the risk of cervical cancer, as Raptor claims?
No, it does not.
The FDA and ‘Surrogate Endpoints’
On the contrary, Raptor’s source confirms what I wrote originally: the FDA approved Gardasil for licensure on the grounds it could prevent cancer despite no clinical studies having demonstrated the truth of this claim. As Raptor’s source observes (emphasis added):
Both vaccines have been shown to be highly effective against HPV16/18–associated cervical intraepithelial neoplasia grades 2 and 3 (CIN2/3) and adenocarcinoma in situ, endpoints accepted in trials for vaccine efficacy against cervical cancer.
That is to say, the FDA used what is called a “surrogate endpoint”, defined as “a biomarker that is intended to substitute for a clinical endpoint”.
As Thomas Fleming explains in the journal Health Affairs (full text here; bold emphasis added),
Establishing that an experimental drug can provide quality-of-life or survival benefit in a newly diagnosed patient with prostate or breast cancer, or that a vaccine can reduce the spread of HIV, or that a device can reduce risk of serious illness or death from cardiovascular disease could require trials that are large, long term, and financially costly.
In many instances, sponsors have proposed alternative endpoints (that is, “surrogates”) for these clinical endpoints, to reduce the duration and size of the trials….
Unfortunately, demonstrating treatment effects on these biological “surrogate” endpoints, while clearly establishing biological activity, may not provide reliable evidence about effects of the intervention in clinical efficacy measures.
Fleming provides the remarkable example of the drugs encainide and flecainide. Since these drugs were shown to be “very effective in suppressing” ventricular arrhythmias, which are “a known risk factor for sudden cardiac death”, the medical establishment assumed that patients who took these drugs would have a lower risk of that outcome.
Fleming continues (emphasis added):
In fact, they were so persuaded that between a quarter-million and a half-million patients each year in the United States alone were receiving these drugs for this purpose. Many were so confident that the drugs provided important therapeutic benefits that they thought it would not be ethical to withhold these drugs from patients in the control group of a randomized controlled trial (RCT) designed to reliably evaluate their effects on overall mortality. (Similar arguments are made today by advocates for continued widespread use of antibiotics in children with acute otitis media, even though we lack scientific evidence to establish that antibiotics meaningfully decrease complications or reduce the time to resolution of symptoms.)
Fortunately, a controlled trial of encainide and flecainide was conducted. The Cardiac Arrhythmia Suppression Trial provided results that astounded cardiologists. These two anti-arrhythmia agents, while suppressing arrhytmias effecively, not only did not provide an improvement in survival, but actually tripled the death rate. Encainide and flecainide may have produced some benefit though [sic, “through”] suppression of arrhythmias, yet they also had unintended and previously unrecognized mechanisms that ultimately led to an adverse effect on overall survival, mechanisms that would not have been detected if there had not been a trial to directly assess the effects on the clinical-efficacy endpoint of overall survival.
This raises an important point I overlooked when writing my rejoinder to Dr. Summers’ Washington Post op-ed: just as important as the question of whether the HPV vaccine actually reduces the risk of cervical cancer is the question of whether the vaccine reduces mortality.
After all, if the vaccine, say, reduces the risk of cervical cancer while increasing the risk of death due to some other cause, then, obviously, it does not follow from the fact that it reduces the risk of cervical cancer that therefore it is a good idea to get the vaccine.
Also, while Fleming cites the example of pediatricians routinely resorting to antibiotics for ear infections, he might just as well have cited the argument given by the medical establishment and public policy defenders for why it would be unethical to do a study comparing autism rates (or other health outcomes, for that matter, such as autoimmune disease) for children vaccinated according to the CDC’s schedule with children who remained completely unvaccinated.
No such study has been done because to withhold the vaccines from children, the argument goes, would be unethical since it would deprive children of the vaccines’ benefits.
Just as those who believed that encainide and flecainide must be effective at lowering mortality based on a surrogate endpoint, so does this argument against doing vaccinated versus unvaccinated studies beg the question. It assumes in the premise the very proposition to be proven (the petitio principii fallacy) — namely, that vaccines given according to the CDC’s schedule are safe and effective.
The DTP Vaccine and Mortality
A stark example of this fallacy is found in the case of the DTP vaccine (which has been replaced in the US with the acellular pertussis vaccine, DTaP, but is still widely used elsewhere around the globe). Since receipt of the vaccine has been shown to reduce the incidence of diphtheria, pertussis, and tetanus, the assumption has been that therefore mass vaccination with DTP will reduce mortality.
In fact, however, what studies show is that the DTP vaccine increases mortality.
The most recent of these, a study published in February of this year in the journal EBioMedicine, stated researchers’ findings bluntly (emphasis added):
DTP was associated with 5-fold higher mortality than being unvaccinated [with DTP]. No prospective study has shown beneficial survival effects of DTP. Unfortunately, DTP is the most widely used vaccine, and the proportion who receives DTP3 is used globally as an indicator of the performance of national vaccination programs.
It should be of concern that the effect of routine vaccinations on all-cause mortality was not tested in randomized trials. All currently available evidence suggests that DTP vaccine may kill more children from other causes than it saves from diphtheria, tetanus or pertussis. Though a vaccine protects children against the target disease it may simultaneously increase susceptibility to unrelated infection.
To return to Raptor’s claim that the Journal of the National Cancer Institute study showed that the HPV vaccine prevents cancer, recall that it in fact confirmed what I had written about the FDA, which relied on a surrogate endpoint in its licensure of Gardasil.
Furthermore, this study in fact confirms what I wrote about why Dr. Summers would be unable to point to any such studies: because none exist.
As Raptor’s own source states, “it may be many years before the effect on HPV vaccination on the incidence of cervical cancer can be assessed.”
Hence we can see that Raptor’s claim that this study showed that the HPV vaccine reduced the incidence of cervical cancer is a bald-faced lie.
It would be superfluous to examine the remainder of the Raptor’s links.
On the Measles Vaccine
“I’m rapidly becoming impatient with Hammond’s arguments”, Raptor informs readers as we come to the next matter I raised in my rejoinder to Dr. Summers: the measles vaccine.
Summers had pointed out that one rare complication of measles is encephalitis, or brain inflammation, and then asked why any parent would risk their child becoming brain damaged by measles “when there’s a safe way of of protecting their children” (referring, of course, to the measles vaccine).
I pointed out that Summers’ statement wrongly implied that encephalitis is not a possible adverse effect of vaccination. I cited a couple of studies in the medical literature that have indicated that encephalitis is a rare outcome of measles vaccination, and I also pointed out that it’s included on the list of possible adverse events on the product insert for Merck’s MMR (measles, mumps, and rubella) vaccine.
Raptor’s response to my observation is to assert that I’m guilty of creating “a false dichotomy – either a vaccine is 100% safe or it’s unsafe”.
It’s Raptor, however, who is here guilty of the fallacy of strawman argumentation. Of course, I neither said nor suggested any such ridiculous thing. I merely observed — accurately — that Dr. Summers was characterizing the vaccine as though it was 100% safe.
Next, Raptor asserts that I think “that package inserts are some sort of infallible document” — another ludicrous strawman. Raptor notes that “a package insert is never evidence of correlation or causality”. That is true, and of course I hadn’t suggested otherwise. I simply observed the fact that encephalitis is listed under the section listing possible adverse events on Merck’s product insert.
So we can see how the very act of stating a fact in a context of questioning public vaccine policy automatically renders the person stating the fact a believer in “pseudoscience”. It’s through such tactics that defenders of public policy attempt to stifle any form of dissent.
Raptor’s next point is a valid one: assuming the three cases of encephalitis reported for every three million doses of MMR given were actually caused by the vaccine, “the risk of encephalitis from measles is still substantially higher than the vaccine”. That is true.
It’s also true that adverse reactions to vaccines are for numerous reasons widely underreported in the Vaccine Adverse Event Reporting System (VAERS), which was also established under the 1986 law granting vaccine manufacturers legal immunity (The National Childhood Vaccine Injury Act).
But both of these facts are beside the point I was making, which is that it is dishonest to characterize vaccination as though it was a medical intervention that entails no risk of any serious harm.
Raptor rightly frames it as a question of weighing benefits versus risks. But this just bolsters my whole point, which is that the public ought to be properly informed of what those risks are rather than told they don’t exist.
In Raptor’s calculation, the benefits of the measles vaccine far outweighs any risks. But that’s a decision that every parent should make for every child with every vaccine. And there are countless other variables to consider to be able to make an informed choice that the public just isn’t being informed about.
For example, parents aren’t being informed that, just as studies show that the DTP vaccine has “non-specific effects” (that is, consequences that are unintended or unexpected) resulting in increased mortality, so have studies long found that natural infection with measles has non-specific effects that are beneficial. Natural infection with the measles virus not only confers lifelong immunity against measles, but also seems to be an important childhood disease that primes the immune system to help protect against other diseases, as well.
Benefits of Getting Measles
“In the 1970s,” as Science Daily notes, “measles infections were observed to cause regression of pre-existing cancer tumors in children.” This observation has led Mayo Clinic to experiment with using measles virus to treat brain cancer.
A study published in The Lancet in 1985 found a negative history of measles to be associated with an increased risk of developing “immunocreactive diseases, sebaceious skin diseases, degenerative diseases of bone and cartilage, and certain tumours.”
A study published in the American Journal of Epidemiology the same year found that infection with measles is associated with a reduced risk of Parkinson’s disease, suggesting “a truly protective effect of measles”.
More recently, a study published in the International Journal of Cancer in 2013 found “a protective role of childhood infectious diseases” — namely measles — “on the risk of CLL [chronic lymphoid leukaemia] in adults”.
A study published in the journal Atherosclerosis in 2015 found that “Measles and mumps, especially in case of both infections, were associated with lower risks of mortality from atherosclerotic CVD [cardiovascular disease].”
Dr. Summers naturally fails to disclose this kind of information in his op-ed so parents could do a proper cost-benefit analysis to determine whether vaccination is right for them.
One begins to see why studies have shown that parents who are choosing not to vaccinate their children, far from being unintelligent or “anti-science”, tend to be well-educated and affluent.
It’s the parents who choose not to put blind faith in an observably corrupt medical establishment that, rather than address their legitimate concerns, has shunned and ridiculed anyone who dares to question public policy, including parents of vaccine-injured children.
It’s the parents who understand how bias can become institutionalized. (No “conspiracy theory” is required to explain how the medical establishment could be wrong, though when it comes to “tobacco science”, there is certainly an element of willfulness. Older generations may recall how advertisements for cigarettes used to feature doctors’ endorsements, and it is not as though there wasn’t an abundance of other examples where the medical establishment has gotten it wrong.)
It’s the parents who are doing their own research, including by doing something most doctors and journalists can’t seem to be bothered with: digging into the medical literature (which can be searched at PubMed.gov) to see for themselves what science actually has to say about vaccines.
Measles and Mortality
Raptor emphasizes that “measles can be a serious illness requiring hospitalization”.
That is true. It is also true that the mortality rate from measles had already plummeted prior to the introduction of the vaccine. This can be seen in the CDC data presented in the below graph (note that the vaccine was licensed in 1963, after the last year shown on this graph).
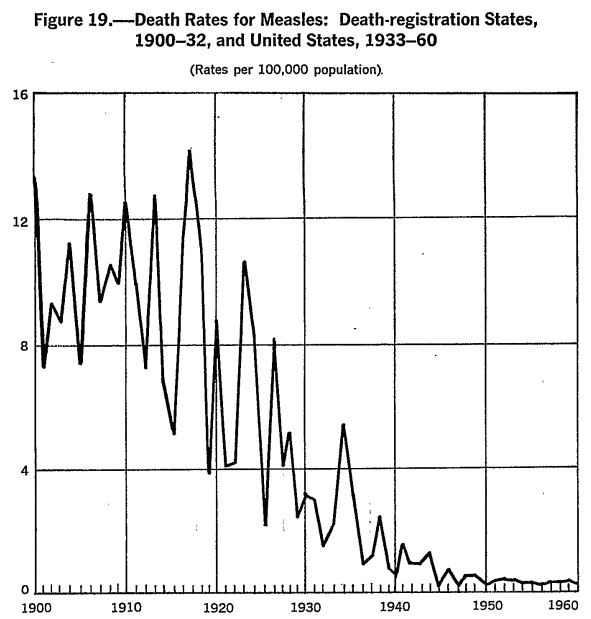
In fact, as an article in the journal Pediatrics notes, “nearly 90% of the decline in infectious disease mortality among US children occurred before 1940, when few antibiotics or vaccines were available.”
Moreover, the risk factors for complications from measles, unlike the risks from the vaccine, are quite well understood — such as malnourishment and, most specifically, vitamin A deficiency.
This brings us to the next objection of Raptor’s to my reply to Summers’s op-ed. Summers had written:
Preventing measles isn’t a matter of avoiding some minor ailment. The disease killed over 100,000 people in 2015.
I replied:
Summers notes the the deaths of over 100,000 people in 2015 as a result of measles infection as though the mortality rate in the US, absent mass vaccination, would be no different than in third-world countries in Africa.
Raptor asserts that I’m “just plain wrong” here; “Dr. Simmons [sic] wasn’t trying to imply that 100,000 children would die in the USA, he’s speaking worldwide.”
But that was precisely my point. Dr. Summers was citing a statistic suggesting a mortality rate that would apply to other countries, but not to the US — a fact which Raptor here tacitly acknowledges.
Raptor claims Summers “wasn’t trying to imply” that the mortality rate of measles would be the same in the US as it would be in developing countries. One might wonder how Raptor can read Summers’ mind, but it makes no difference because it isn’t a question of intent. Whether intentionally or not, Summers did in fact imply just that.
In fact, it was in this very same paragraph that Summers noted that there is a risk of brain damage from measles and asked, “Why on earth would parents opt for that risk when there’s a safe way of protecting their children?”
Summers was, of course, directing his question specifically toward American parents when he wrote that.
Raptor’s next comment is, “Of course, Hammond’s point sounds vaguely offensive that somehow only Africans will die of measles, and not privileged white Americans. Sigh.”
So now, in addition to it being “anti-science” to point out the acknowledged fact that the mortality rate in the US would not be the same as in developing countries, it is also “offensive” to point out that Americans enjoy a higher standard of living.
Sigh.
Unintended Population Effects of Mass Vaccination
Among other factors that aren’t taken into consideration in the risk-benefit analysis underlying public policy are unintended effects at the population level. For example, one effect of mass vaccination for measles is that in the event of an outbreak today, the risk burden has shifted away from children in whom it is a generally mild disease onto those for whom it poses a greater risk of complications: infants.
This is because in the pre-vaccine era, most women experienced measles infection as a child and developed a robust cell-mediated immunity. Frequent reexposure to the virus also kept antibody levels high. Since antibodies are passed from mother to baby via breastmilk, breastfeeding provided a strong passive immunity to infants, who do not yet have a developed immune system to be able to handle the infection on their own.
Now, however, thanks to mass vaccination, mothers aren’t as well able to confer immunity to their infants via breastmilk. This is because the immunity conferred by the vaccine isn’t as robust as that conferred by natural infection and wanes more quickly over time, and by reducing the circulation of the virus, the natural boosting of antibody titers from frequent reexposure no longer occurs.
Thus, because mothers in the era of mass vaccination aren’t as well able to pass protective antibodies on to their infants via breastmilk, in the event of an outbreak, infants are at a higher risk.
Conclusion
Raptor closes by describing my response to Summers’ op-ed as consisting of “tropes, myths, conspiracy theories, cherry picking and, need I mention this, outright misinformation.”
It is fitting that Raptor should close with such words because, in the end, having failed to identify even a single error in fact or logic in anything I wrote, such empty rhetoric is all Raptor has got. Rather than reasonably addressing my points, Raptor resorts to misrepresentation, strawman argumentation, obfuscation, and ad hominem attacks.
I am perfectly content to let intelligent readers decide for themselves, therefore, who is more “anti-science”.
Such efforts to bully and intimidate people into conformity will ultimately fail, but there’s a lesson in it: to dare to question public vaccine policy is a sin for which one must be rebuked.
It is to commit the crime of heresy against the vaccine religion.
The heretics, however, will not be intimidated.
We will not be silenced.
Original article was reprinted with permission in its entirety. Jeremy R. Hammond is an award-winning independent journalist, author, publisher and editor of Foreign Policy Journal, and father. Subscribe to stay updated with his work on vaccines and get his free report “5 Horrifying Facts about the FDA Vaccine Approval Process.”
We received permission to published it from The World Mercury Project.
Source Article from http://feedproxy.google.com/~r/Collective-evolution/~3/G5MlNo2J_n4/
Related posts:
Views: 0
 Posted in
Posted in  Tags:
Tags: 
















